























-
A&P Ultrasound Training
-
Clinical Ultrasound Training
-
Adv. Clinical Ultrasound Training
-
U/S-Guided Procedure Training
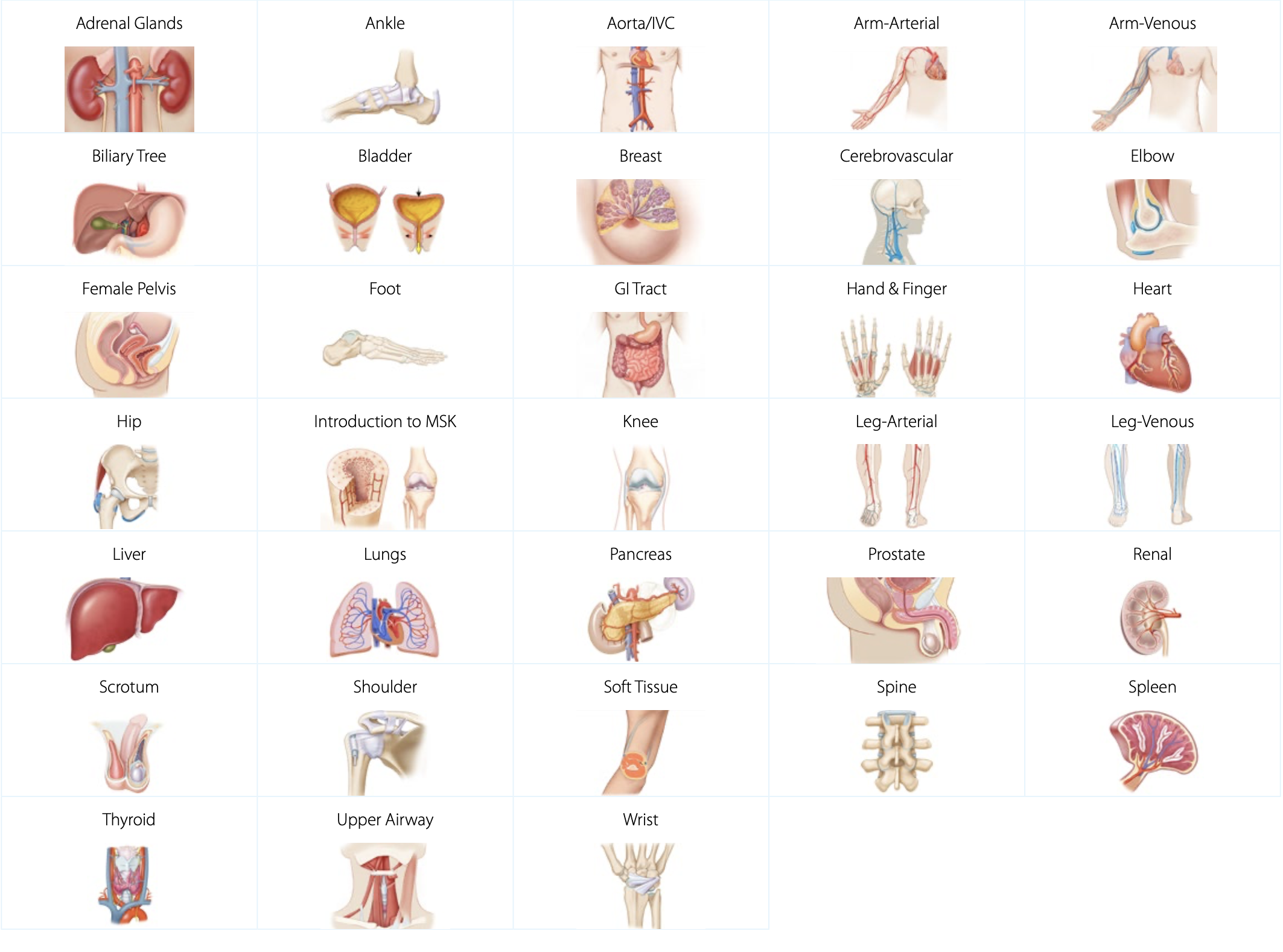
Anatomy & Physiology Ultrasound Training
Our A&P ultrasound training provides a strong foundation of ultrasound knowledge, specific to anatomical regions, organs, and structures. Our expert-led ultrasound training covers everything from regional anatomy & physiology to sonographic anatomy, scanning technique, and imaging tips & pitfalls. Each topic comes with relevant scanning cases from real patients applied to virtual patients, available to scan in the SonoSimulator. Our A&P training comes with normal sonographic cases to set the baseline of normal sonographic anatomy.
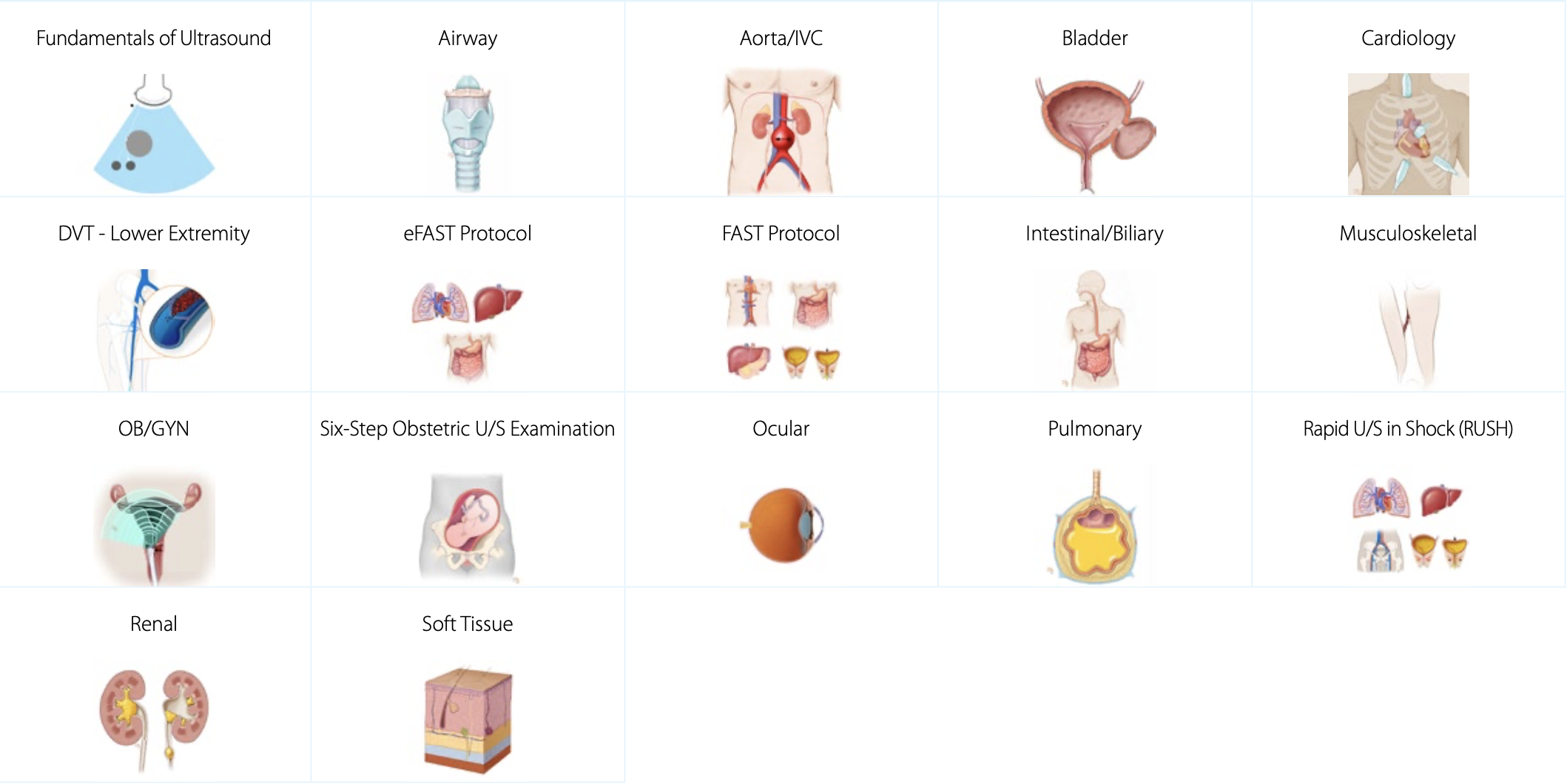
Clinical Ultrasound Training
Our clinical ultrasound training provides the necessary components to accurately assess and diagnose using ultrasound. We cover exam indications, regional anatomy, sonographic anatomy, and sonographic technique. These training topics also focus on pathologic case studies and imaging tips & pitfalls to give you an in-depth understanding of how diseases present in ultrasound imaging. Each topic comes with 10-20 real pathologic scanning cases pertinent to the learning objectives for each topic. Learners can scan these cases in the patented SonoSimulator.
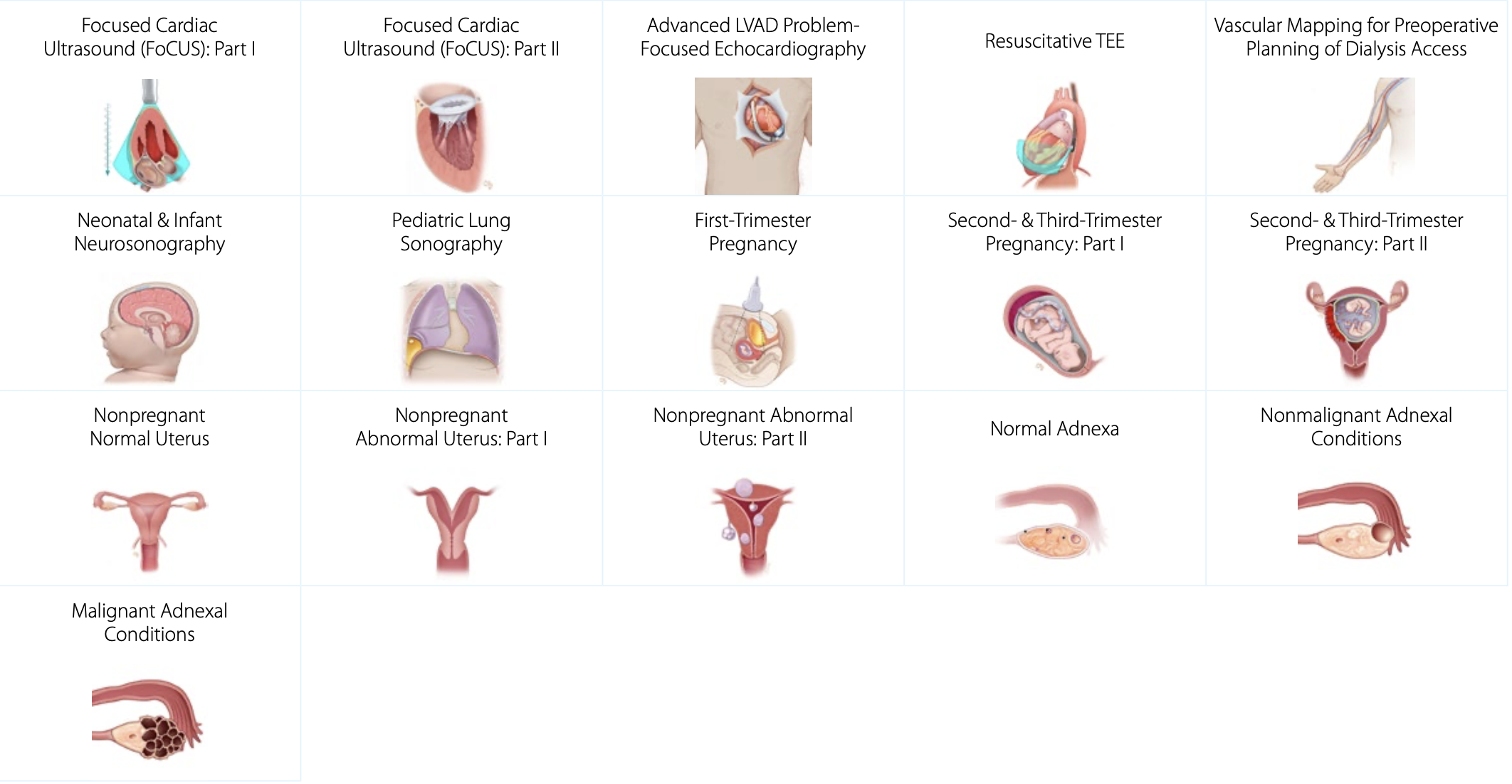
Advanced Clinical Ultrasound Training
Our advanced clinical ultrasound training covers complex diagnoses and sonographic applications. This is an ever-expanding list of topics with a focus on specific pathologic conditions. These advanced clinical and diagnostic ultrasound topics provide learners with a deep understanding of ultrasound techniques for assessing a variety of complex medical conditions. These topics also come with 10-20 real pathologic scanning cases that learners can access and scan with the SonoSimulator.
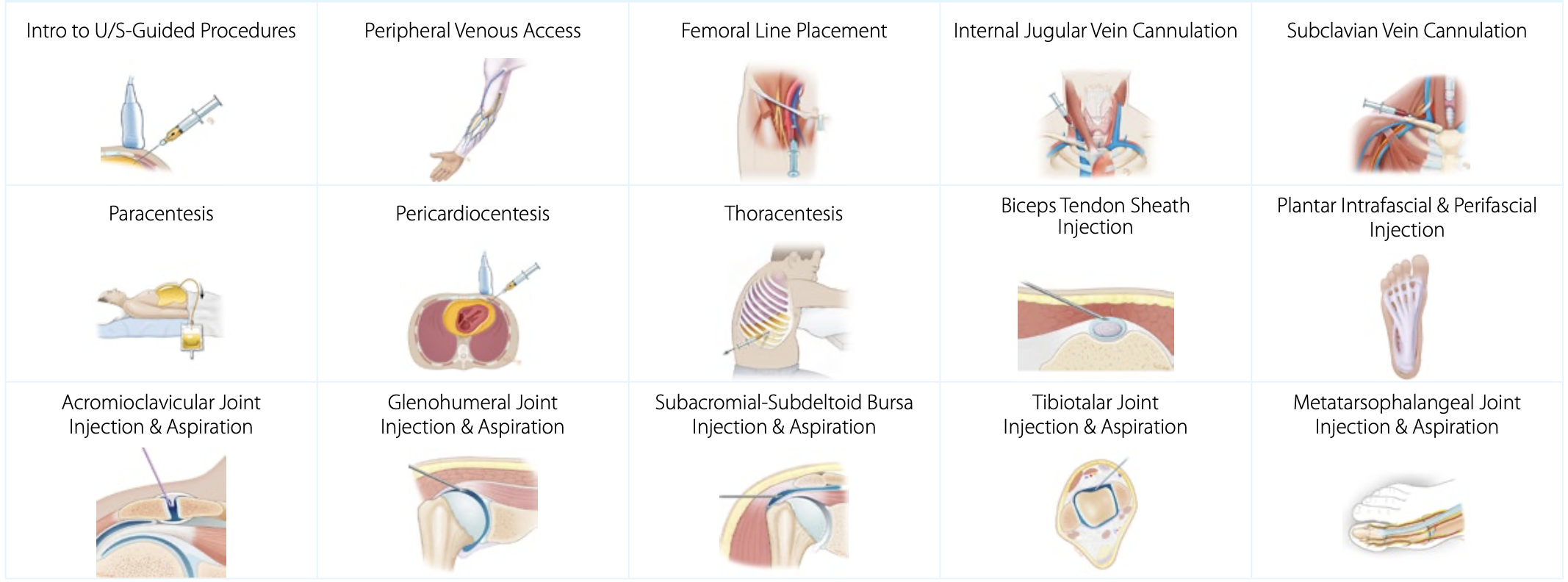
Ultrasound-Guided Procedure Training
Ultrasound-guided procedures are becoming increasingly used to minimize complications and improve patient care. SonoSim ultrasound procedures training covers patient positioning, procedural steps, imaging adjuncts, potential complications, and more. Learn at your own pace in a risk-free environment. Practice ultrasound-guided procedures as often as you like, risk-free - anytime, anywhere - on any laptop, with the SonoSimulator.
