





-
Anatomy & Physiology
-
Core Clinical
-
Advanced Clinical
-
U/S-Guided Procedures
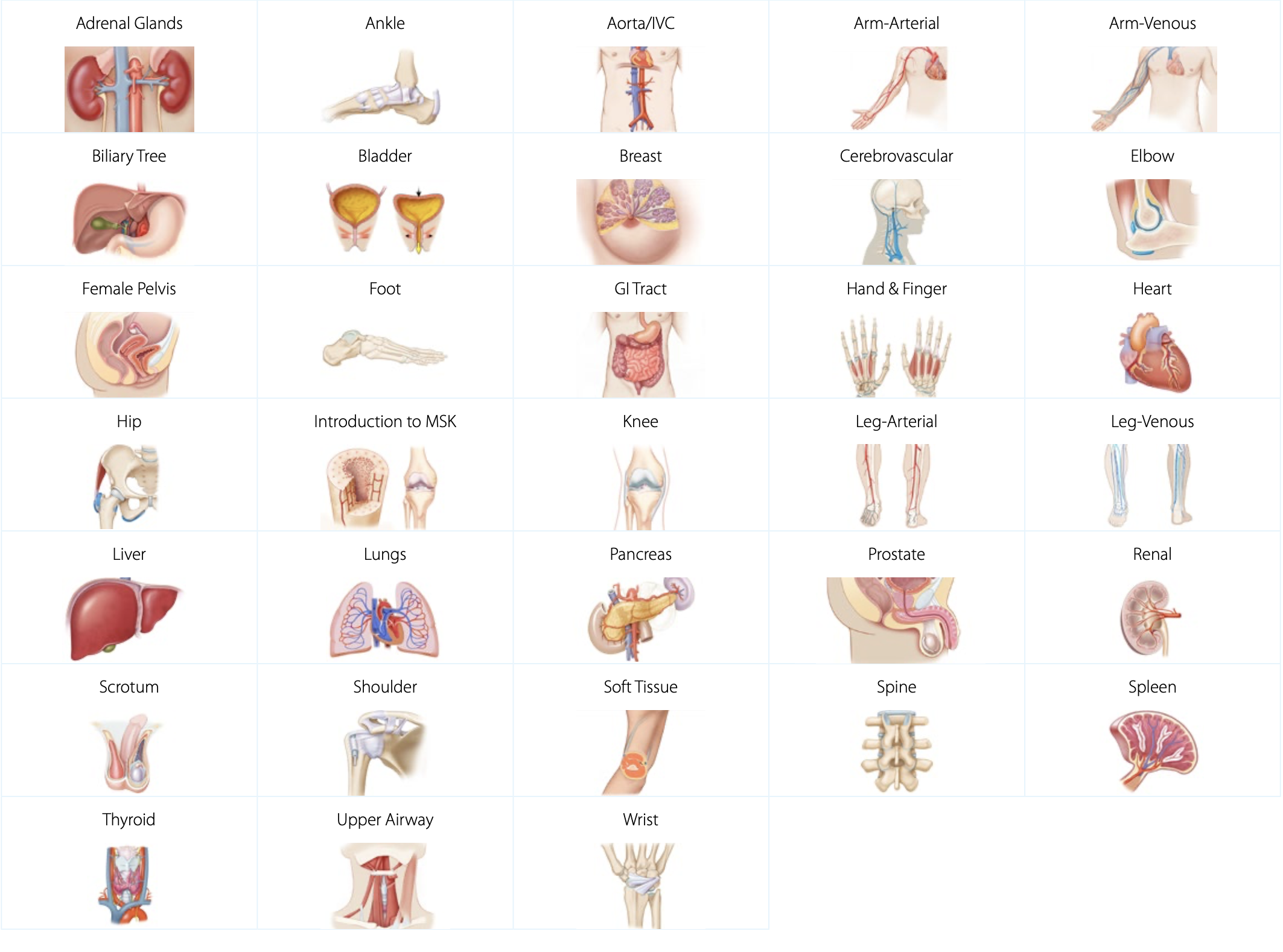
Anatomy & Physiology
SonoSim Anatomy & Physiology topics provide a strong foundation of ultrasound knowledge, specific to anatomical regions, organs, and structures. Developed by ultrasound experts, SonoSim training covers regional anatomy & physiology, sonographic anatomy, scanning techniques, and imaging tips & pitfalls. Each topic comes with several scanning cases that are accessed in the SonoSimulator to reinforce learning from the courses with hands-on scanning on real patient ultrasound imagery.
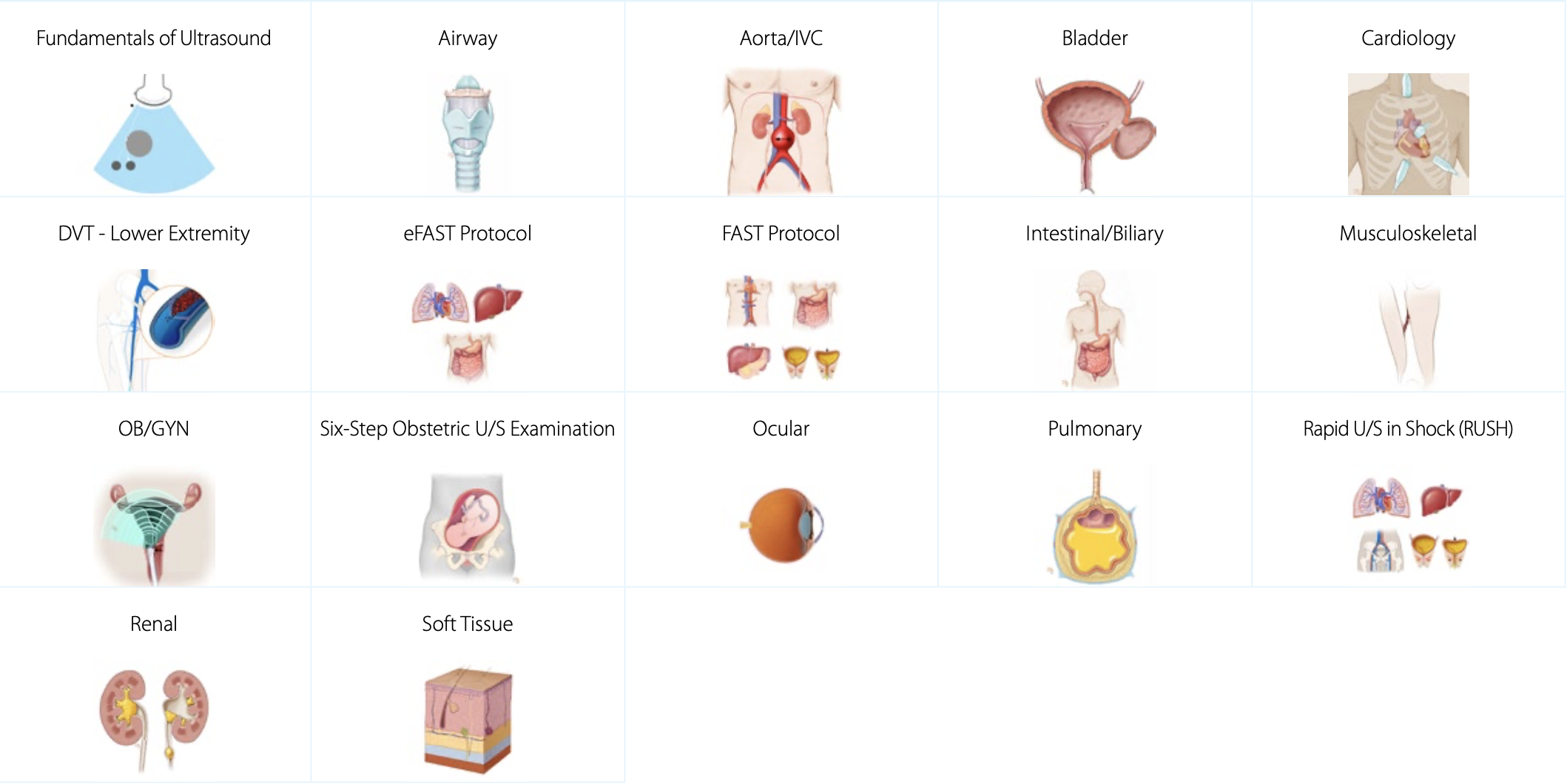
Core Clinical Ultrasound Courses
Our Core Clinical Ultrasound Courses provide an in-depth understanding of the components required to accurately assess and diagnose using ultrasound. Exam indications, regional anatomy, sonographic anatomy, and sonographic technique are covered. There is a focus on pathologic case studies and imaging tips & pitfalls. These courses are ideally suited to prepare your point-of-care ultrasound (POCUS) learners for simulation scenarios.
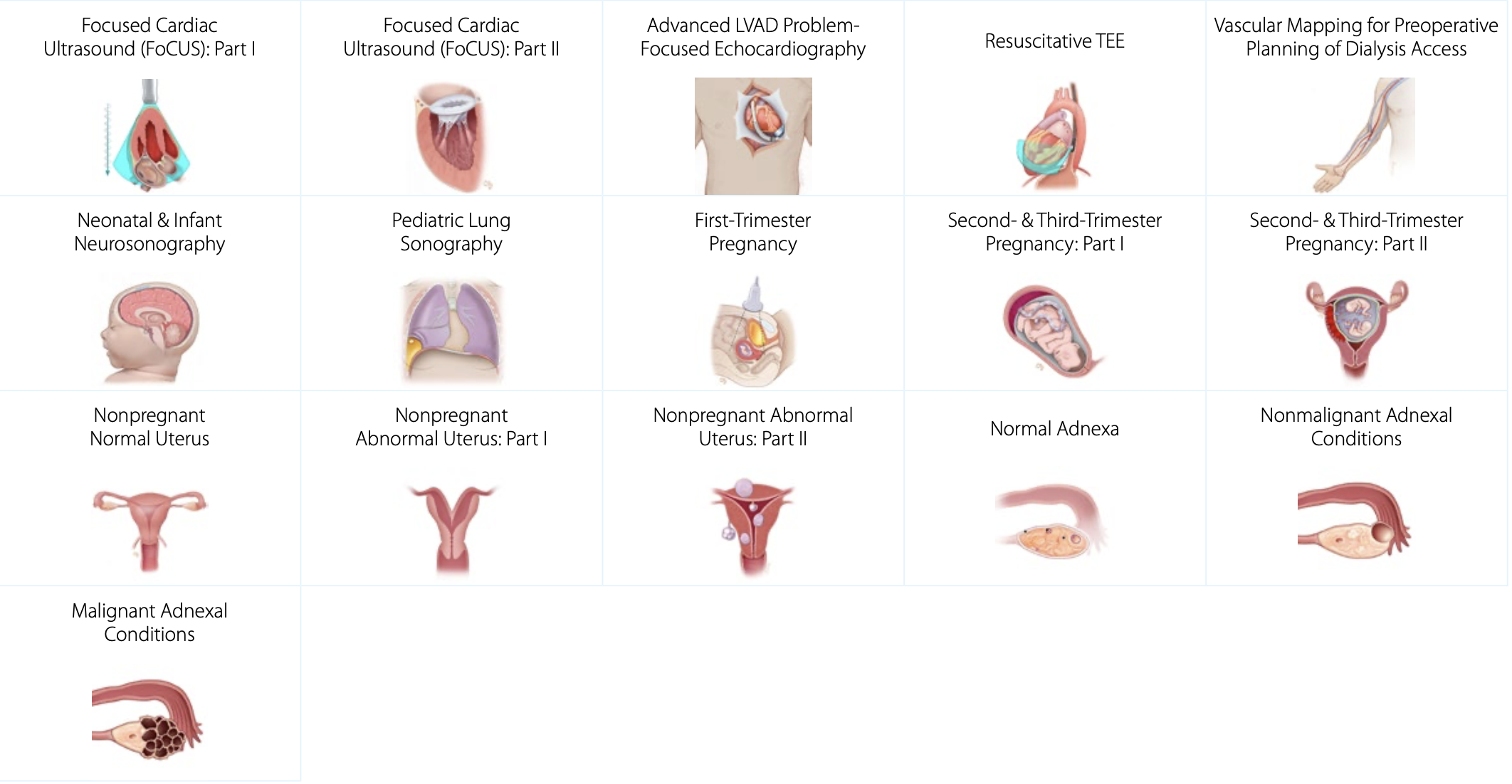
Advanced Clinical Ultrasound Courses
SonoSim Advanced Clinical Ultrasound Courses cover complex diagnoses and sonographic applications. With a focus on specific pathologic conditions, these advanced clinical and diagnostic ultrasound topics provide learners with a deep understanding of ultrasound techniques for evaluating various complex medical conditions.
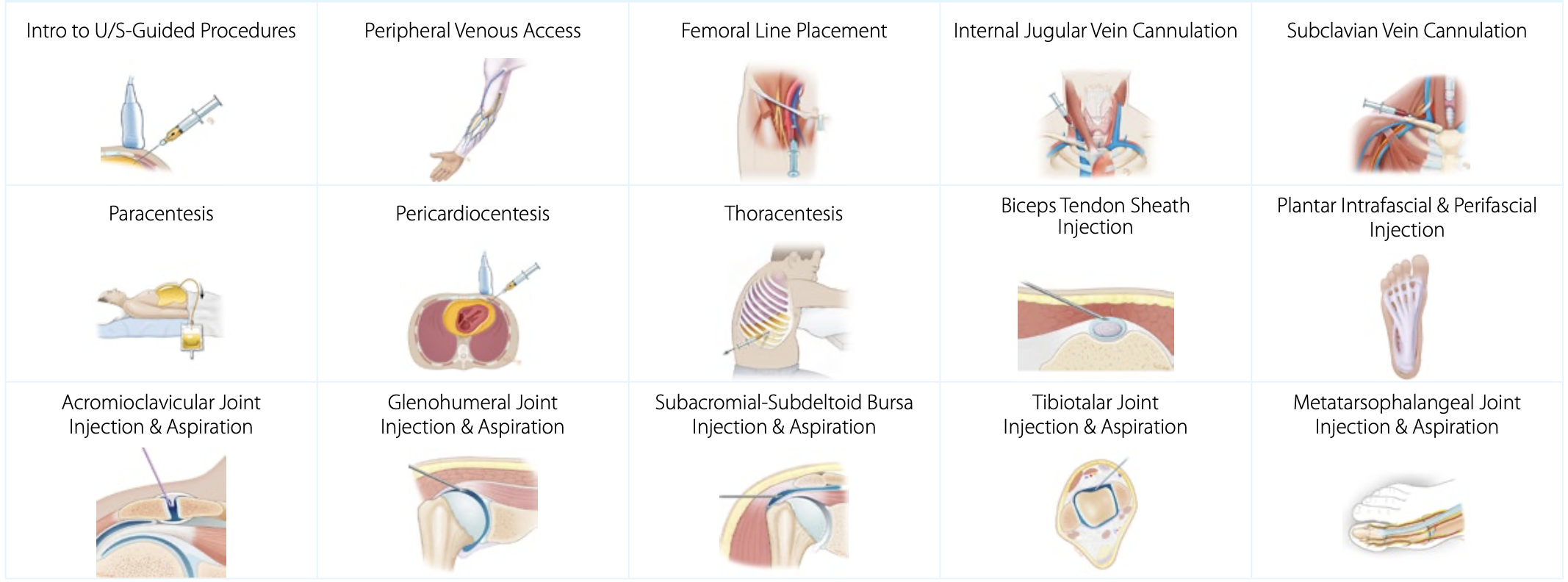
Ultrasound-Guided Procedure Courses
SonoSim ultrasound-guided procedure courses cover patient positioning, procedural steps, imaging adjuncts, potential complications, and more. Using real patient data sets that vary in body morphology, right versus left-sided approaches, and pathophysiologic states, SonoSim helps prepare learners for in-person Sim Center sessions using phantoms and ultrasound machines.






















-
Critical Care
-
Emergency Medicine
-
Family Medicine
-
Internal Medicine
-
OB/GYN















